Semaglutide vs Tirzepatide is one of the most important GLP-1 research comparisons today. Both compounds appear in metabolic research, but they do not work in the same way.
Semaglutide acts as a GLP-1 receptor agonist. Tirzepatide acts on both GLP-1 and GIP receptors. Because of this, researchers often compare their receptor action, half-life, trial data, and dose-planning needs.
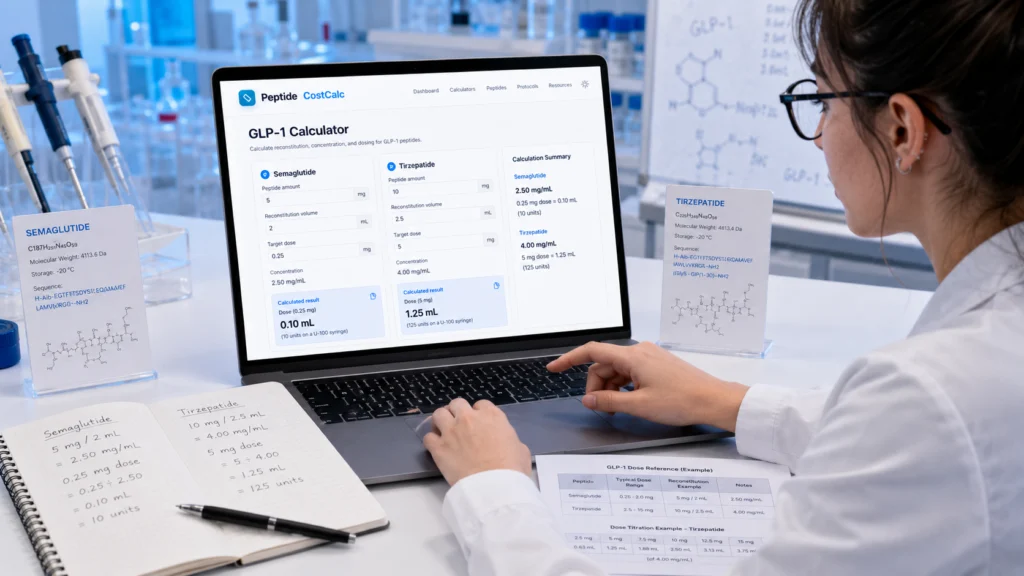
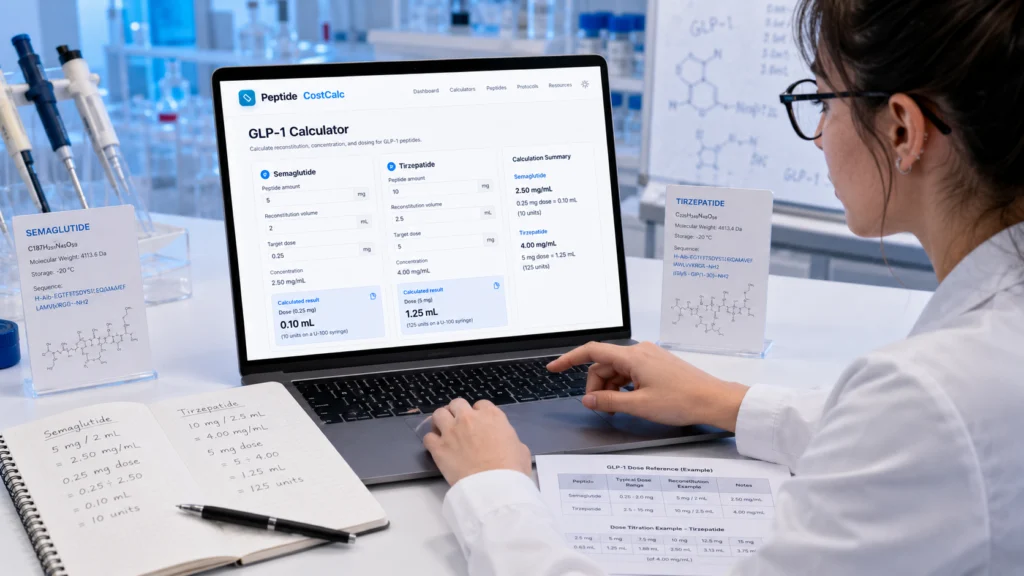
For calculation support, researchers can use the free GLP-1 Semaglutide & Tirzepatide Calculator on Peptide CostCalc.
Quick Comparison on Semaglutide vs Tirzepatide
| Point | Semaglutide | Tirzepatide |
|---|---|---|
| Receptor action | GLP-1 receptor agonist | Dual GIP and GLP-1 receptor agonist |
| Research focus | Glucose control, appetite signalling, gastric emptying | Glucose control, appetite signalling, GIP/GLP-1 interaction |
| Approximate half-life | About 1 week | About 5 days |
| Study style | GLP-1-only model | Dual incretin model |
| Calculator use | Weekly dose and vial planning | Weekly dose and vial planning |
The Main Mechanism Difference
The biggest Semaglutide vs Tirzepatide difference is receptor activity.
Semaglutide targets the GLP-1 receptor. This receptor plays a role in insulin secretion, appetite signalling, and gastric emptying. The FDA Wegovy label notes that semaglutide has an elimination half-life of about one week.
Tirzepatide works differently. It activates both the GIP receptor and the GLP-1 receptor. The FDA Mounjaro label notes that tirzepatide has a half-life of about five days.
This dual action makes tirzepatide a different research compound, not just a stronger version of semaglutide.
What the Research Shows
The SURPASS-2 trial compared tirzepatide with semaglutide in adults with type 2 diabetes. In that study, tirzepatide showed greater reductions in HbA1c and body weight than semaglutide 1 mg.
Weight-focused studies also show strong interest in both compounds. The STEP 1 trial reported major weight reduction with semaglutide 2.4 mg over 68 weeks. The SURMOUNT-1 trial reported larger average reductions with higher tirzepatide doses over 72 weeks.
However, researchers should not treat separate trials as a perfect direct comparison. Study design, dose, population, and duration all matter.
Why GIP Matters
GIP stands for glucose-dependent insulinotropic peptide. It is another incretin hormone.
Tirzepatide’s GIP and GLP-1 activity is the main reason researchers study it separately from semaglutide. The dual-receptor model may help explain why tirzepatide performs differently in some metabolic endpoints.
This area still needs careful study. Researchers should focus on receptor biology, trial design, and measurable endpoints instead of simple “better or worse” claims.
Dose Planning and Calculator Use
Both compounds often need careful calculation in research planning. Researchers may need to check vial size, reconstitution volume, weekly dose, syringe volume, and total compound needs.
The GLP-1 Semaglutide & Tirzepatide Calculator helps convert GLP-1 values into practical calculation outputs. It can support vial planning, syringe-volume estimates, and schedule checks.
For general peptide calculations, researchers can also use the Peptide Dosage Calculator and the Peptide Half-Life Calculator.
These tools provide mathematical estimates only. They do not replace professional judgment or medical advice.
 Final Takeaway on Semaglutide vs Tirzepatide
Final Takeaway on Semaglutide vs Tirzepatide
Semaglutide vs Tirzepatide is mainly a comparison of receptor design. Semaglutide works through GLP-1 receptor activation. Tirzepatide works through both GIP and GLP-1 receptor activation.
This difference affects how researchers compare mechanisms, half-life, study outcomes, and dose-planning needs.
For simple research calculations, use the free GLP-1 calculator on Peptide CostCalc. It helps turn compound, vial, and dose values into clear calculation outputs.
Helpful Research Links
For primary reference data, researchers can review the official and published sources below:
Wegovy FDA label for semaglutide half-life
Mounjaro FDA label for tirzepatide half-life
SURPASS-2 tirzepatide vs semaglutide trial
STEP 1 semaglutide trial
SURMOUNT-1 tirzepatide trial